 Hospital Commissioner Meeting 3/19/2014 (Audio Only)
Hospital Commissioner Meeting 3/19/2014 (Audio Only)
During this board meeting, I presented the following 2 proposals to the board:
Proposal 1: Define Board Expectations for Collections Practices and Policies
This board has defined and often talked about what our expectations are for how this public hospital district conducts medical care, but we have not given similar clear guidance regarding our expectations of our financial services.
I think it will be helpful moving forward, if we add to our Ends goals a clear statement characterizing our expectations for how this hospital district financially impacts the lives of our patients and their families. With this in mind, I propose we add to the Boards ends policy the following:
The Jefferson Healthcare billing, charity care, and collections policies and practices will be fair, reasonable, and as compassionate as possible, within the limits of the law and available resources.
After we agree to this amendment, we can then begin discussing how to monitor the districts effectiveness in achieving it. But the first step is simply stating our end goal.
Proposal 2: Board Monitoring use of 3rd party Collections Activities
My 2nd proposal is that this hospital board immediately begin monitoring the use of 3rd party collections companies by this hospital district.
A collections monitoring report will serve to help monitor several board policy goals including those in finance, patient satisfaction, public image, community health.
I know the Jefferson Healthcare financial counselors strive to work with patients to come up with affordable solutions. But, when this does not work out-for any reason, patients may end up sent to collections on a medical debt they cannot afford- and the consequences of this are severe. These consequences include:
The patients credit getting damaged.
The patient being subjected to extraordinary collections actions – in the name of Jefferson Healthcare but without the direct oversight of Jefferson Healthcare staff.
The patients learning to view Jefferson Healthcare as an adversary rather than as a partner and steward of healthcare in our community.
The patient learning that seeking healthcare will have severely negative financial consequences- and so they stop seeking it promptly when needed- putting their future health at higher risk, and contributing to the likelihood of expensive yet preventable emergency care in the future. (Note: if the patient is unable to afford the emergency care bill, the public will end up paying for it- at a much higher cost than the cost of the initial preventative care.)
I know my fellow commissioners want Jefferson Healthcare to relentlessly strive to be a partner and steward of our communities health and by monitoring our collections activities we will gain a valuable perspective into how well we are doing towards this goal.
I recognize this hospital district has a fiduciary responsibility to act to collect debts. But I also recognize that its mission is not to maximize profits at the expense of the health of our community. Our mission is to serve as compassionate partners in the health of our community- and this means we must be particularly mindful of any actions we take that may in fact harm community members.
So, due to the significant consequences in the realms of finance, customer satisfaction, community health, and public image- that result when sending a patient account to collections, I propose we immediately begin taking steps to monitor data related to our use of these 3rd party collection services.
I recommend we begin by reviewing as soon as possible a detailed study of Jefferson Healthcare collections practices including the following data:
Trends and totals for:
Total number of open accounts currently held by 3rd party collection agencies.
Monthly # and % of patients sent to collections.
Monthly total money recovered through collections agencies.
Monthly total money written off despite use of collection agencies.
Annual trends and totals for these same items going back 5 years.
After we review the data, I will then recommend we immediately discuss setting clear goals and guidelines related to it.
I also repeated the following proposal I made at the 3/5/2014 meeting:
Publish Board Bylaws and Policies Online
Jefferson Healthcare immediately publish the most current versions of our hospital board policies and bylaws on the hospital district website for easy review by the general public.
Below is a transcript of the verbal exchange about the board policies and bylaws proposal. This was basically a discussion on whether or not we wanted to discuss the idea. There was no support for a 2nd for my motion to consider this proposal, so we did not officially consider it. (According to Roberts Rules of Order the way a board action works is 1- someone makes a motion, 2- someone seconds the motion, 3- Discussion of the motion, 4- Vote). If you wish to listen to the dialogue it is at the 01:46:30 mark! :
C. Ready: Last meeting I asked if there was interest in publishing our policies and bylaws online. There was some thought that you would like to think about it. I was wondering if there is anyone that is interested in discussing putting our board policies and bylaws online?”
C. Dressler: I think this would come again at the April…because we don’t have anything we’re going to put up at the moment because we’re going through reviews and revisions and the decision as to what form of governance. So that’s my personal take on it. So I don’t know what you…
C. Deleo: I believe I recommended at the last meeting that we wait on publishing that until we have the final out of our rewrite. I think publishing one and then a month later publishing a second one could be confusing.
C. Dressler: And do you have any comment Chuck.
C. Russel: No. I agree with Tony.
C. Ready: Personally, I think it’s…they are our current policies and I think it is reasonable to put the current policies that we’ve been operating under up. But I sense I am not going to get a second to that motion.”
Hospital Commissioner Meeting 3/5/2014
 I don’t have a full record of the March 5, 2014 commissioner meeting, but I do want to share several items I brought up to the board during the board business portion of the meeting. Please note, these are not exact quotes, but are paraphrased from my recollection and the statements I had prepared and brought with me to the board meeting.
I don’t have a full record of the March 5, 2014 commissioner meeting, but I do want to share several items I brought up to the board during the board business portion of the meeting. Please note, these are not exact quotes, but are paraphrased from my recollection and the statements I had prepared and brought with me to the board meeting.
Item 1: Board Policies and Bylaws Transparency
The first issue I raised was regarding the publication of board policies and bylaws on the hospital district website. I said something to this effect:
“I think it is important that this board operate in a transparent and open manner so that the public can best understand what we are doing and why we are doing it. With this in mind, I think we should publish our board policies and bylaws online. These documents inform virtually every action and decision this board touches upon during these commission meetings. Moreover, I know we are considering revising these documents and as such, isn’t it appropriate for the public to understand the current policies so they can appreciate our discussions of how to change them? I would like to know my fellow commissioners thoughts on this.”
The other commissioners made some remarks, but I do not have their exact words, so I do not want to attempt to paraphrase them in case I misunderstood. We did not take action on this suggestion during this meeting.
Item 2: March 21 Special Session Questions
Next, in reference to the March 21st special session I said:
“I believe the March 21st special session is largely being scheduled in response to my request for information and discussion which I stated during our board retreat and at the following board regular session. With this in mind, I wanted to make certain everyone understood clearly what questions I am hoping for us to focus upon. I am more than happy to meet with and work with the facilitator who is planning that special session to help make this happen. My questions are:
- What is the current organizational view of community health needs- which it has been using to guide major policy and decision making including the ESS building project?
- What is the current organizational priorities amongst these recognized community health needs?
- How will the new building project impact/ benefit the community? (This might be titled a “Community benefit Analysis” or “Community Health Needs Impact Analysis”)
- What will be our mechanism’s for evaluating the building project’s effectiveness regarding community benefit?
- What are the building projects measurable objectives re community benefit?”
The other commissioners made some remarks, but I do not have their exact words, so I do not want to attempt to paraphrase them in case I misunderstood.
Item 3: Community Health Needs Questions
The 3rd major issue I raised were questions about the Community Health Needs Assessment which the hospital is participating in collaboration with the Health Department. I said:
I propose we formalize in policy this organizations relationship to community health needs assessments. I think this will help us moving forward.
Questions we will benefit from asking and answering clearly include:
- Why are we participating in a community health needs assessment?
- Who is responsible/accountable for the successful completion of a community health needs assessment?
- Is the community health needs assessment important for the board to effectively govern and for JHC leadership to successfully strive to fufill the hospital districts mission?
- How often should a community health needs assessment be done?What is to be done with the community health needs assessment upon completion? Based on my research, there are 3 things that can happen after a community health needs assessment. First and most common is NOTHING. This, Dr. Locke reminded us is far too often the result. But the two very positive constructive things that can happen are a Community Health Improvement Plan, which would be done in collaboration with other community stake holders, and a community benefits report, in which the hospital would clearly state its plans to take action to positively impact the health needs of the community. Which of these choices will we make?
- Will we participate in a community health improvement plan process? If so, how often? Who will do it? How will it’s effectiveness be monitored and evaluated?
- Will we require a community benefit plan be drafted for JHC? If so, how often? Who will do it? How will it’s effectiveness be monitored and evaluated?
- Does the current JHC mission statement adequately affirm that our policies integrate and reflect the public interest in our meeting our responsibilities as a public hospital district? In other words, does our mission statement clearly state our simple responsibility to “identify and meet the healthcare needs of our community?
I have found some models used in other healthcare institutions that answer the above questions which I am considering consolidating into an amendment proposal for this board to consider.
There was no discussion following the above remarks.
Item 4: Charity Care and Collections Policies
Regarding hospital charity care and collections practices I said,
“I have some concerns that our charity care and collections policies and practices are not as fair and reasonable as they could be- and as the board might expect them to be. I met with a private citizen this past week who had done some interesting research into our collections practices and it was very thought provoking. I suspect we have some strong opportunities for improvement. I also think it is appropriate for this board to set very clear expectations about our hospital district charity care and collections policies, perhaps even if it is merely to say, “The charity care and collections policies of this hospital district will be fair, reasonable” and perhaps even “compassionate.” With this in mind, I am considering drafting an amendment to our board Ends policies regarding our charity care and collections practices and how we might monitor such expectations.”
There was no discussion following the above remark.
Next Commission Meeting: March 19, 2014
I will keep this blog updated as I continue to work with the commission towards action on the items above and more.
This Blog is About to Wake up!
It has been an exciting several months for me since my election was confirmed in November. I have been learning a lot and I continue to work very hard to understand everything I need to understand so that I can work as hospital commissioner to help make healthcare better and accessible to everyone in our community.
In addition to many hours of independent study and research, I have of course attended a large number of meetings in my new role as commissioner including both regular commission meeting sessions and otherwise. The many discussions I have engaged in have also helped me learn and evolve my thinking and approach to healthcare in our community. I have lost none of my excitement and determination to work to make things better, but I have gained far more clarity on the exact steps needed to begin to earnestly make more headway towards affordable high quality healthcare for everyone. With this in mind, I have decided to utilize this website to make clear to anyone interested what is happening and what I am focused upon in my role as hospital commissioner.
I hope you find this helpful and informative.
Election Results!
11/8/2013 update: Near final count is in. I am now ahead 402 votes and they tell me: I win! Thanks again to everyone who did anything to support me. This has been an incredible experience. I will work to make everyone proud to have me as a hospital commissioner!
11/6/2013 update: I am currently ahead 202 votes. There are probably about 2000 ballots still to arrive in the mail. The next count will happen Friday around noon. Thank you so much to everyone who supported me! I needed every single one of you to get to this point! A few more days of waiting to see perhaps a definitive result.
Understanding the Impact of the Affordable Care Act
This video does a great job explaining the scope and impact of the Affordable Care Act. It recognizes that millions of people will continue uninsured, but unfortunately, it fails to highlight the critical problem of underinsurance. Insurance is not a guarantee of affordable access to care because deductibles and copays are often barriers to care.
So the picture below from the video, should look like this:

So what do we do? We need our public hospital district and our health department to recognize that they are the last line of defense to make sure people in our community get the care they need. We need to monitor access, explore options for expanding it through local programs, and relentlessly advocate for single payer/universal healthcare at the state and national level. The ACA allows states to implement a single payer system in 2017, we should work with Rep. Sherry Appleton to make that happen. Single payer is the only way to affordably ensure all people comprehensive access to healthcare.
State Representative Sherry Appleton Endorses Matt Ready for Hospital Commissioner
On August 22 I met with Washington State Representative Sherry Appleton to discuss how we can work together to ensure all people have affordable access to healthcare. Representative Appleton is the sponsor of a bill to make Single Payer/ Universal Healthcare a reality in Washington State (HB 1085 Washington Health Security Trust). I believe every hospital commissioner in every public hospital district in Washington State should be engaged in the single payer discussion as it is the only way to stop out of control healthcare costs and bring comprehensive healthcare to all people.
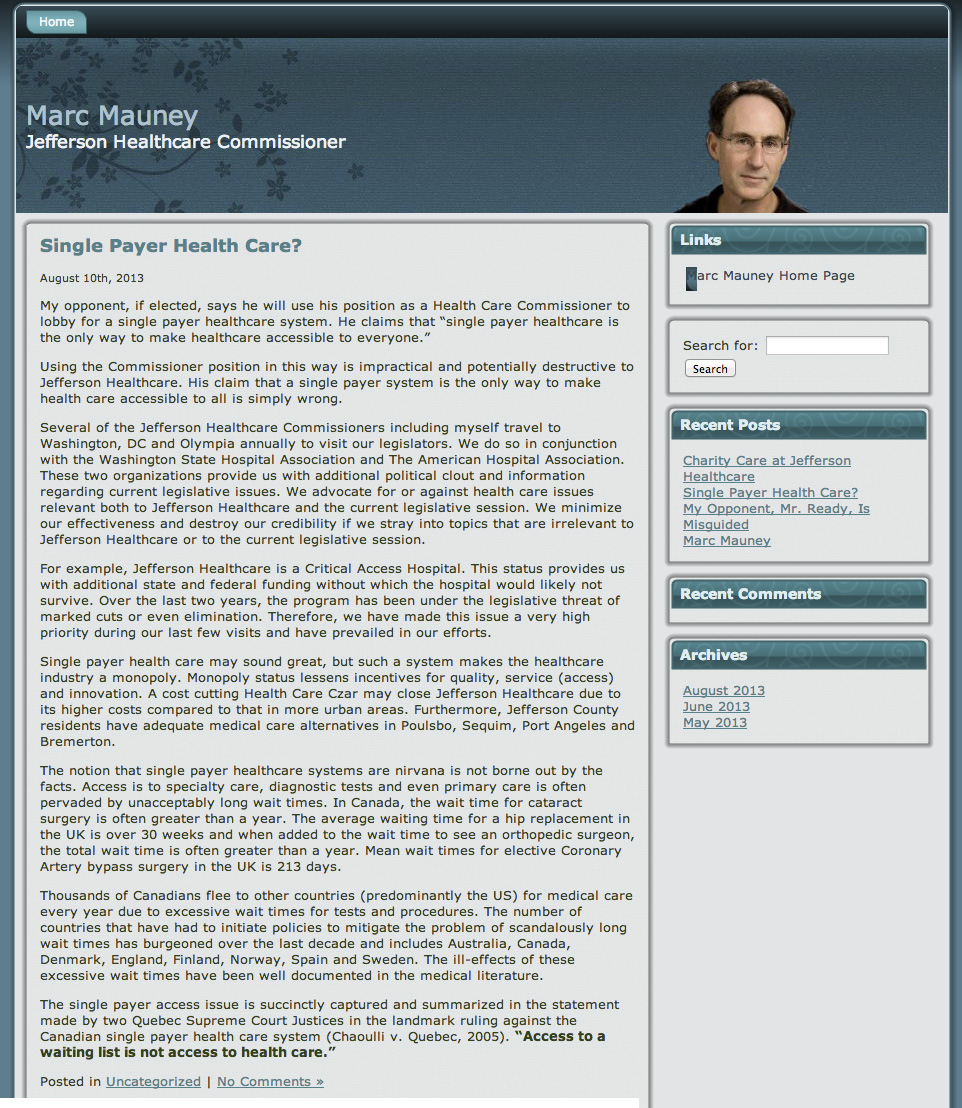
My opponent is opposed to single payer healthcare. He seems to believe in a profit driven healthcare system. His solution is continue a system that limits care to those who cannot afford it, rather than risk longer wait times. If you would like to learn why 13,000 physicians disagree with my opponent, please visit Physicians for a National Health Plan. Here is his statement on single payer. If you wish to help my campaign, please write letters of support to the editor of the Peninsula Daily News and the Port Townsend Leader. You can also request a yard sign, a meet and greet, or make a donation using the links on this page.
Candidates Matt Ready and Savannah Hensel Ask Jefferson Healthcare Board to Make Access a Top Priority
http://readyforhealthcare.org – On July 3, 2013 I spoke at a Jefferson Healthcare Hospital Commission meeting and asked the board to respond to the problem of healthcare access by taking the first step of making it a documented top goal in the Jefferson Healthcare Strategic Plan. Here is the video of my comment, their responses, and the followup comment from Hospital Commissioner Candidate Savannah Hensel.
I ask you declare healthcare access a top priority of this district, add it to the strategic plan, and set an aggressive goal for us to improve it.
A brief summary of the dialogue:
Matt Ready: The strategic plan is a great accomplishment, but it has something critical missing- access. Access is a problem in our community- and across our nation. 14-29% of the residents of our district are delaying or not seeking healthcare due to financial barriers. This is a serious problem with serious consequences. The ultimate solution is universal single payer healthcare- which I hope you advocate for when you meet with our State and Federal representatives, but you don’t have to stop there. Our hospital district can follow the lead of other local public institutions like San Francisco, Howard County Maryland, and Snoqualmie Valley Hospital and develop our own innovative solutions to make healthcare affordable and accessible for more people. We should be working to make healthcare financially accessible to 100% of our community- but we won’t do it if we don’t try. We won’t try unless you make it a goal of our district. You have the power to make it a goal and push us to work on this. I ask you declare healthcare access a top priority of this district, add it to the strategic plan, and set an aggressive goal for us to improve it.
Summary of Responses from Mike Glenn, Jill Buhler, Marc Mauney, and Tony Deleo:
- Absolutely, access is a top priority of the commission and all of administration. Everyone agreed to this…yet
- It is unnecessary and redundant to put access in the JHC Strategic plan- since we already focus on access in everything we do (like breathing).
- Jefferson Healthcare already does more than other hospitals since we don’t turn anyone away- and this is good enough.
- The Affordable Care Act will expand Medicaid and create more subsidies for people to buy private insurance, so we should wait and see how well that helps improve access.
- If people are not coming to Jefferson Healthcare due to cost, then that is their fault. JHC doesn’t “bar the doors” or turn anyone away. We constantly tell everyone in our community to come in, even if they cannot pay.
- Years ago, the Jefferson Healthcare Board of Commissioners considered two major actions to improve access:
- Creating an affordable access program with KPS that would give people a way to have catastrophic insurance coverage, pay JHC a small stipend, with the guarantee they could get all their medical needs met at Jefferson Healthcare at a reasonable affordable cost. This initiative was stopped when the State Insurance commissioner said it was “illegal”.
- Creating a larger free healthcare clinic similar to the one at Olympic Medical Center. This was voted down by at least one commissioner because he didn’t want people to have the indignity of having to go to a separate facility if they lost their job and insurance.
Matt Ready: In response to Commissioner Buhler description of the affordable access program that was considered but never implemented, I remarked that that is exactly the type of innovative thinking we could be doing right now to improve access. Maybe there was a way around the roadblock created by the State Insurance Commissioner.
Savannah Hensel: Savannah asked if in the last 10 years any of the Hospital Commissioners had experienced life without health insurance and without financial access to healthcare. (No commissioners responded.) Savannah then shared that she has spend 95% of her adult life without health insurance and without the ability to afford her hospital bills despite the sliding scale policies of the hospital. She said she knows what it is like to not have access due to the financial barrier and she seconded the request the Jefferson Healthcare make access a top 5 priority and add it immediately to the Strategic plan.
There were no further responses and the meeting adjourned.
Conclusion
This was a great opening dialogue with the hospital commission about access! It is obvious all the commissioners care about access, the problem is they either think access is not a problem or that the hospital district is already doing everything it should be doing. At a future commission meeting I will address some of the reasons they think this way and continue to challenge them to recognize the opportunity for helping make healthcare more accessible to all people in our community.
Anyone who has any thoughts, questions, or comments about this please feel free to contact me at readyforhealthcare@gmail.com or use our contact form.
Update!
Here is a sneak peek at what I will be saying (my current rough draft) in response to the Board’s concerns at the next commission meeting:
At the last commission meeting I asked you to declare access to healthcare a top priority of this hospital district, add it as a top 5 priority in the Strategic Plan, and challenge us to work towards an aggressive goal for improving it.
I received a number of thoughtful responses- although overall I would summarize your response as:
You agree access is a top priority, but you feel you are already doing everything appropriate in that realm, and there is no need to add it to the strategic plan. Tony even went so far as to say it would be like reminding employees to breath- since access is always considered in our decisions.
I work in performance improvement. It is my job to help directors, leaders, departments, and staff solve problems. When I am called into a meeting about a problem, the first step is always working together to clearly define the problem- and agreeing to clear metrics for measuring the problem. If you don’t do that, then you are not all speaking the same language.
You and I are not currently speaking the same language about access.
Is access a problem in this hospital district? If it is, how big of problem is it? Is it more or less of a problem than it was 2 years ago? How are you answering these questions?
Several of you said, this hospital is more generous than any other hospital district in the state. That may be true- but is that good enough? Maybe sometimes being the best is not good enough.
Several of you said in essence that access is not a problem since we don’t turn anyone away. As Tony said, we don’t bar the doors. If they aren’t coming, that is their choice.
I applaud you for having a policy more generous than other hospital districts. I applaud you for not denying people health care if they cannot afford it. But remember, what do we do if someone gets care here and cannot afford their portion of the bill- even after we adjust their bill for sliding scale? What do we do? We collect on them. We pressure them to pay just like any private corporation would. Those who cannot pay what we judge they should, we send to collections. We don’t close our doors to anyone- and if you cannot pay your portion of your bill, we will send you to collections. That is the current state of access at Jefferson Healthcare. Yes, it may be better than other hospital districts- but that doesn’t mean it is good enough. This is one area, where I think you should stop comparing yourself to your peers, and start looking more closely at this problem in your community.
We offer access to healthcare to people who cannot afford it like a credit card company offers access to money- we are happy to give it to you- but we will come after you for it. When given that choice- the people who cannot afford healthcare suffer. They suffer when they struggle to pay their bill. They suffer when we pressure them. They suffer when they are sent to collections. They suffer when they choose to delay or avoid care altogether because they don’t want to go into debt.
How do you know if healthcare access is a problem or not? To know, you have to define it and measure it. That takes some serious thoughtful conversations that will not happen in this brief public comment period of the commission meeting. But you can make these serious thoughtful conversations happen- if you as our leaders declare it a priority.
It doesn’t mean you are committing to any specific action, all I am saying is make us delve into this, make us figure out how we measure access, make us report to you the state of access, and then decide if there is a problem. Then you will have a measure to monitor. Tony said, if the ACA falls apart, then we will do something. How will you know if the ACA is working or not if you aren’t measuring anything?
If you declare it a priority- and put it in strategic plan, that sets the gears of improvement energy in motion. That forces us to be accountable to this goal. I know- as this is what I do at Jefferson Healthcare. The strategic plan drives our focus- as it should.
As I said last time, if you look at this, you will see a serious problem- a great opportunity to help our community.
Thank you.
Why Do I Strongly Advocate for a Single Payer System (Universal Healthcare)?
I advocate for a single payer healthcare system because it is the best solution to the costly and inequitable healthcare system we have in the US currently. As a nation we pay twice as much as other industrialized countries for our healthcare, yet we get less coverage and cover only a portion of our population. Below is a chart illustrating these facts:
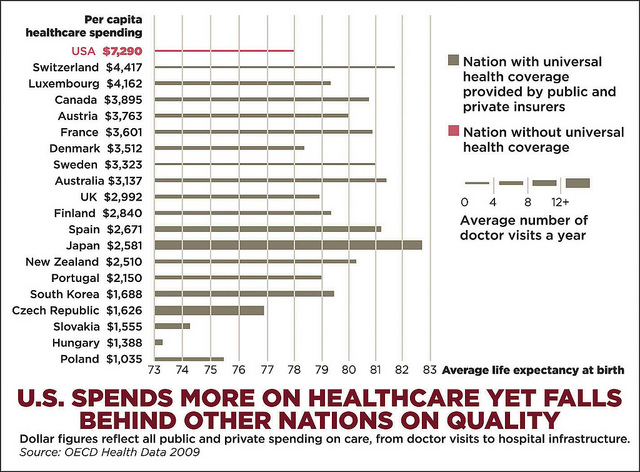
As you can see, in the US, we spend far more, we get fewer doctor visits per year, and we have lower life expectancies than other countries with universal healthcare. Single payer should not be a partisan issue. Rather, it should be recognized as a critical step towards improving US Healthcare. Below are some of my favorites statements for single payer healthcare reform:
Physicians for a National Health Plan
Single-payer national health insurance is a system in which a single public or quasi-public agency organizes health financing, but delivery of care remains largely private.
Currently, the U.S. health care system is outrageously expensive, yet inadequate. Despite spending more than twice as much as the rest of the industrialized nations ($8,160 per capita), the United States performs poorly in comparison on major health indicators such as life expectancy, infant mortality and immunization rates. Moreover, the other advanced nations provide comprehensive coverage to their entire populations, while the U.S. leaves 51 million completely uninsured and millions more inadequately covered.

The reason we spend more and get less than the rest of the world is because we have a patchwork system of for-profit payers. Private insurers necessarily waste health dollars on things that have nothing to do with care: overhead, underwriting, billing, sales and marketing departments as well as huge profits and exorbitant executive pay. Doctors and hospitals must maintain costly administrative staffs to deal with the bureaucracy. As a result, administration consumes one-third (31 percent) of Americans’ health dollars, most of which is waste.
Single-payer financing is the only way to recapture this wasted money. The potential savings on paperwork, more than $400 billion per year, are enough to provide comprehensive coverage to everyone without paying any more than we already do.
Under a single-payer system, all Americans would be covered for all medically necessary services, including: doctor, hospital, preventive, long-term care, mental health, reproductive health care, dental, vision, prescription drug and medical supply costs. Patients would no longer face financial barriers to care such as co-pays and deductibles, and would regain free choice of doctor and hospital. Doctors would regain autonomy over patient care.
Physicians would be paid fee-for-service according to a negotiated formulary or receive salary from a hospital or nonprofit HMO / group practice. Hospitals would receive a global budget for operating expenses. Health facilities and expensive equipment purchases would be managed by regional health planning boards.
A single-payer system would be financed by eliminating private insurers and recapturing their administrative waste. Modest new taxes, based on ability to pay, would replace premiums and out-of-pocket payments currently paid by individuals and business. Costs would be controlled through negotiated fees, global budgeting and bulk purchasing.
David May, MD, PhD
April 23, 2013
I am a Republican. For those who know me that is not a surprise. I live in a red state. I have never voted for a Democratic presidential candidate. I can field strip, clean and reassemble a Remington 12-gauge pump blindfolded. And on top of it, I think we should talk about having a single payer national health care plan. The reason is quite simple. In my view, we already have one; we just don’t take advantage of it.
Firstly, Medicare and the Center for Medicare and Medicaid Services (CMS) are de facto setting all of the rules now. They are a single payer system. When we go to lobby the Hill, we lobby Congress and CMS. Talking to Blue Cross, Aetna, Cigna and United Health care is essentially a waste of time. All the third party payers do is play off the Medicare rules to their advantage and profit. They have higher premiums, pay a somewhat higher benefit and have a significantly higher level of regulation which impedes the care of their customers. This is no longer consumer choice but effectively extortion, a less than hidden shake down in which the “choice” for a family of four is company A at $900 per month or company B at $1100 per month. The payers are simply taking advantage of the system, playing both ends against the middle.
Secondly, in order to move forward with true health care finance we need complete transparency in cost and expense… and we need it now. As was noted in a recent Time magazine piece on the hidden cost of health care, our current system is a vulgar, less than honorable construct more akin to used car sales than medical care, cloaked under the guise of generally accepted accounting principles and hospital cost shifting.
Thirdly, with a single payer system would potentially come real utilization data, real quality metrics and real accountability. The promise of ICD-10 with all of its difficulties is that of a much more granular claims-made data. We could use some granularity in health care data and we will never achieve it in big data quantities without a single payer system.
Lastly, I think that the physicians should be in charge of health care and not the insurance companies and hospital systems. With a single price structure, it becomes all about medical decision making, efficiency, the provision of care to our patients, and shared decision making, all of which we do well.
How, you might say, could a Republican come to such a position? The simple answer is I really think it is quite Republican. Oh, I know there will be many raised eyebrows and many critics. I accept that. I understand the fact that no single payer system is perfect, that it is “socialist,” that it is “un-American.”
I would submit to you, however, that it is un-American to allow many of our citizens to be uninsured, that it is un-American to shunt money away from a strong military in order to support a bloated, inefficient and fraud-laden health care system, that it is un-American not to be open and above board with the cost of what we do, the expense of that service and the profit that we make. Mostly, it is un-American to let this outrageous health care injustice continue.
– http://blog.cardiosource.org/post/i-am-a-republican-can-we-talk-about-a-single-payer-system-2/
President Richard Nixon, (Republican)
Feb 6, 1974
One of the most cherished goals of our democracy is to assure every American an equal opportunity to lead a full and productive life.
In the last quarter century, we have made remarkable progress toward that goal, opening the doors to millions of our fellow countrymen who were seeking equal opportunities in education, jobs and voting.
Now it is time that we move forward again in still another critical area: health care.
Without adequate health care, no one can make full use of his or her talents and opportunities. It is thus just as important that economic, racial and social barriers not stand in the way of good health care as it is to eliminate those barriers to a good education and a good job.
…These gaps in health protection can have tragic consequences. They can cause people to delay seeking medical attention until it is too late. Then a medical crisis ensues, followed by huge medical bills–or worse. Delays in treatment can end in death or lifelong disability…
Early last year, I directed the Secretary of Health, Education, and Welfare to prepare a new and improved plan for comprehensive health insurance. That plan, as I indicated in my State of the Union message, has been developed and I am presenting it to the Congress today. I urge its enactment as soon as possible.
The plan is organized around seven principles:
First, it offers every American an opportunity to obtain a balanced, comprehensive range of health insurance benefits;
Second, it will cost no American more than he can afford to pay;
…Under the Comprehensive Health Insurance Plan, a doctor’s decisions could be based on the health care needs of his patients, not on health insurance coverage. This difference is essential for quality care.
Every American participating in the program would be insured for catastrophic illnesses that can eat away savings and plunge individuals and families into hopeless debt for years. No family would ever have annual out-of-pocket expenses for covered health services in excess of $1,500, and low-income families would face substantially smaller expenses.
…Comprehensive health insurance is an idea whose time has come in America.
There has long been a need to assure every American financial access to high quality health care. As medical costs go up, that need grows more pressing.
– http://www.kaiserhealthnews.org/stories/2009/september/03/nixon-proposal.aspx

{kind=link}
Conclusion
We already pay enough in taxes to fund a national single payer healthcare system– but we don’t get it.
We need to start having genuine dialogues about healthcare and I believe that can start at the local level. How is the current healthcare system effecting you and your neighbor? How many people in our community are suffering without financial access to healthcare? What can we do at the local level to alleviate this problem? I believe if local communities, hospital districts, cities, and counties begin actively and aggressively grappling with this challenge – we can develop innovative solutions and a lot of suffering might be eliminated. Moreover, this work will help clarify the benefits and need for a State or National single payer healthcare system.